
Ejaculation comes as the outcome of sexual arousal and normally takes place simultaneously with orgasm. As the nervous system gets stimulated, it forwards peristaltic contractions of the muscles in the epididymis and ductus deferens (vas deferens). A small volume of fluid containing semen stored in the epididymis, vas deferens and ampulla of vas deferens is guided towards the prostate urethra. There, it gets mixed with secretions of the seminal vesicles and prostate. The overall secreted fluid, 3-5ml in volume, flows towards the urethra and, finally, the contractions of the bulbocavernous and femorocavernous muschles result in the expulsion of semen from the external urethral orifice.
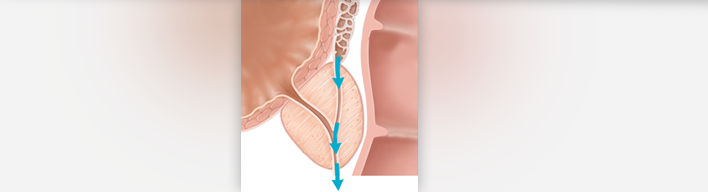
Ejaculation
Ejaculation comes as the outcome of sexual arousal and normally takes place simultaneously with orgasm. It is triggered by the stimulation of the sympathetic autonomous nervous system, which causes peristaltic contractions of the epididymal and vas deferens muscles. A small volume of fluid containing semen stored in the epididymis, vas deferens and ampulla of vas deferens is guided towards the prostate urethra. There it gets mixed with the 2-3ml of alkaline fluids secreted by the seminal vesicles, while the prostate muscles contraction adds 1-2ml milky slightly acidic prostate fluid. The overall fluid, 3-5ml in volume, flows towards the urethra and the contractions of bulbocavernous and femorocavernous muschles ultimately result in the expulsion of the semen through the urethral orifice.
Premature Ejaculation (PE)
Thyroid diseases and mainly hyperthyroidism are today the only known organic diseases to have premature ejaculation as a symptom. As long as the thyroid disease is regulated, the problem is restored. The only pharmaceutical treatment recommended for premature ejaculation is with antidepressant agents, the so-called SSRIs (Selective Serotonin Reuptake Inhibitors).
In all other cases, premature ejaculation is due to psychological causes and is treated by a Sexologist. This is almost the rule for all young men during their first sexual experiences. However, for some of them the problem continues, whereas for others the problem may recur later on in the life. Physicians have not yet fully clarified the mechanism of this phenomenon. Controlling ejaculation can be learnt In exactly the same way as one learns how to control urination (retain or release urine). If there is no ability to control ejaculation, then the man may face a problem. The causes of premature ejaculation though have not yet been fully clarified.
It is almost impossible to provide an accurate definition for premature ejaculation. A large scientific study has demonstrated that:
- The average length of time before ejaculation in men with PE is 1,8 minutes.
- The average length of time before ejaculation in men without any problem is 7,3 minutes.
However, in the study there were men who could have a duration of even 25 minutes, but who supported that they still have premature ejaculation. This clearly shows that people have different perceptions of what actually 'normal' is. Clinical experience indicates that most couples with duration less than 5 minutes feel annoyed, at least in half of their sexual intercourses.
In case one feels annoyed from the fact that ejaculation comes too fast, then he could ask for help.
Within the therapeutic context, the man -and later on the couple- gets trained following some exercises that help to control ejaculation. The couple has to follow a program of special drills that "are tailored" to meet the individual couple's needs. Drills are practised by the couple at home and during herapeutic sessions the Expert evaluates their course and progress and resolves any potential difficulties and problems arising. The aim is always for the couple to fulfil the desired target. These drills have low success rate when not done under the systematic guidance of a Sexologist. In some cases, there may be need for pharmacotherapy to be combined with the exercise program.
Retrograde Ejaculation
During ejaculation, the bladder neck normally closes down so that the semen does not flow into the bladder and cause retrograde ejaculation. Retrograde ejaculation occurs in most men who have undergone prostatectomy for benign prostate hyperplasia. On the contrary, in patients who have undergone radical prostatectomy for prostate cancer, there is absence of ejaculation even though orgasm may maintain. A similar phenomenon can be observed in patients with benign prostate hyperplasia taking drugs for achieving better urination.
Anejaculation
Anejaculation (inability to ejaculate) may also occur after surgical operations if ejaculation nerves have been destroyed. Also, when there are neurological causes or psychological inhibitory factors. In addition, some pharmaceutical agents (mainly psychiatric drugs) are connected with this disorder.